
Managing supplements inside a clinical setting is not a solved problem. Fragmented documentation, missed interaction checks, and inconsistent adverse event reporting create real safety and compliance risks for patients and practitioners alike. A well-designed clinical supplement workflow, which the industry also refers to as a structured supplement administration workflow or pharmacovigilance-integrated supplement protocol, closes those gaps systematically. This guide walks you through the tools, steps, troubleshooting strategies, and performance metrics that transform supplement management from an afterthought into a reliable, audit-ready clinical process.
Table of Contents
- Key Takeaways
- Building a clinical supplement workflow from the ground up
- Step-by-step supplement integration into clinical practice
- Troubleshooting common workflow pitfalls
- Measuring workflow effectiveness over time
- My perspective on where this work actually breaks down
- Supplements your clinical workflow can actually rely on
- FAQ
Key Takeaways
| Point | Details |
|---|---|
| Start with EHR integration | Linking supplement recommendations to your EHR medication workspace improves safety visibility and ordering convenience. |
| Standardize documentation upfront | Protocol templates and data completeness checks prevent authorization delays and compliance gaps before they occur. |
| Automate adverse event reporting | A structured intake-to-MedWatch submission process keeps your team on the right side of FDA timelines. |
| Track adherence actively | Digital dispensary data reveals gaps in patient follow-through before they compromise clinical outcomes. |
| Prepare for new data standards | FDA’s ICH E2B(R3) mandate takes effect October 2026, requiring updated electronic submission infrastructure. |
Building a clinical supplement workflow from the ground up
Before you can standardize anything, you need to know what you are working with. Most clinical settings manage supplements across at least three disconnected systems: verbal or printed recommendation logs, a separate ordering platform, and a manual or EHR-adjacent documentation file. That fragmentation is where errors originate.
The tools that matter most in a structured supplement administration workflow are:
- EHR integration platforms such as Fullscript connected to Epic, which enable direct supplement recommendations through the medication workspace alongside home delivery for patients
- Digital dispensaries that provide real-time adherence data, auto-refill options, and built-in interaction alerts
- Decision support modules that flag supplement-drug interactions, contraindications, and missing documentation fields before a recommendation is finalized
- Structured documentation templates capturing diagnosis codes, clinical rationale, dosage, duration, monitoring plan, and relevant comorbidities
The regulatory layer matters just as much as the technology layer. FDA requires MedWatch Form 3500A submissions within 15 business days for serious adverse events from labeled manufacturers, packers, and distributors. That 15-day clock starts at initial intake, not at investigation completion, so your intake process must be fast, structured, and clearly assigned.
One more compliance date to put on your calendar: starting October 1, 2026, FDA mandates ICH E2B(R3) electronic data standards for postmarketing individual case safety reports submitted via ESG NextGen. If your current submission infrastructure does not support that format, the time to upgrade is now.
Pro Tip: Build a one-page data completeness checklist specific to your supplement protocols, covering all fields required for FDA compliance and internal audit. Flag incomplete entries at the point of documentation, not during monthly review.
The table below summarizes the core tools and their primary functions in a supplement management workflow:
| Tool | Primary Function | Compliance Benefit |
|---|---|---|
| EHR-linked dispensary (e.g., Fullscript + Epic) | Recommend, order, and monitor in one system | Reduces fragmentation; supports coordinated care |
| Decision support module | Interaction checks, contraindication flags | Prevents unreported adverse events |
| Structured documentation template | Captures all clinical and regulatory data | Satisfies FDA recordkeeping and MedWatch requirements |
| Digital dispensary adherence tracker | Monitors patient fill and refill behavior | Enables proactive clinical follow-up |
| ICH E2B(R3)-ready submission system | Electronic adverse event reporting | Meets upcoming FDA mandate |
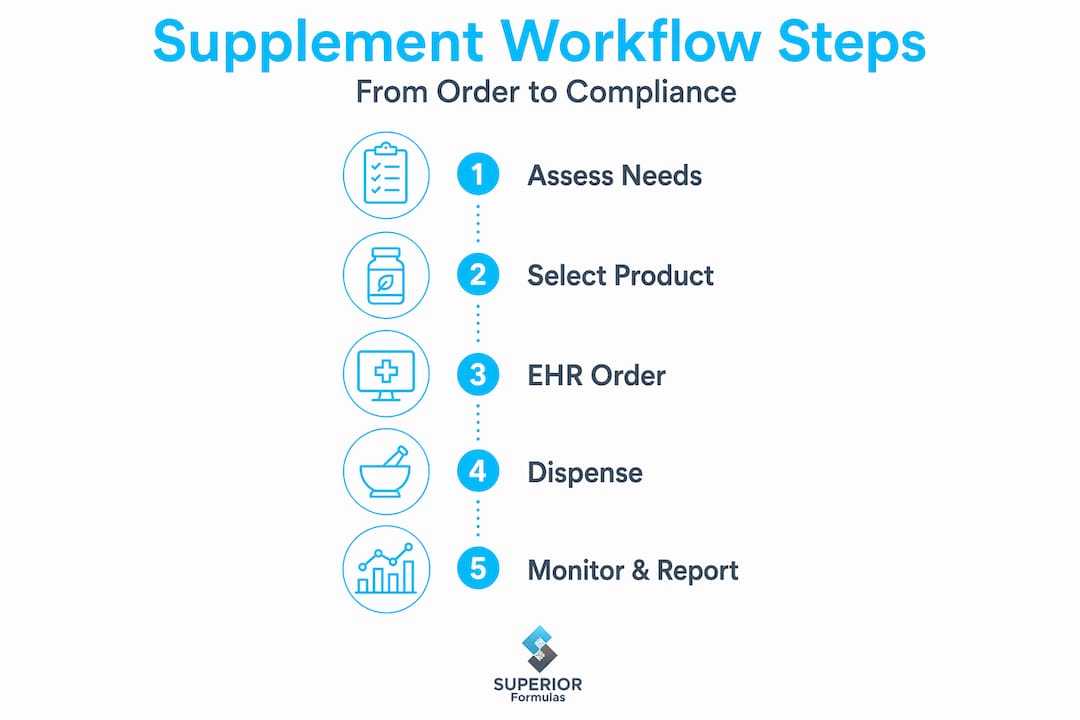
Step-by-step supplement integration into clinical practice
A process is only as reliable as its design. These steps reflect how high-performing clinical teams move from inconsistent supplement management to a protocol-driven, traceable system.
-
Audit your current process. Map every touchpoint where supplements are currently recommended, documented, ordered, and reviewed. Identify where data is missing, duplicated, or siloed. This audit becomes the baseline against which you will measure improvement.
-
Standardize documentation templates by protocol type. Create supplement-specific templates for your most common use cases, such as post-bariatric surgery nutrient repletion, oncology supportive care, or metabolic health protocols. Each template should function as a clinical checklist, capturing indication, contraindications, dosing rationale, and monitoring criteria. Protocol templates improve consistency and reduce the cognitive load on practitioners during high-volume visits.
-
Integrate supplement recommendations into your EHR medication workflow. Treating supplements as external consumer purchases is the single biggest source of safety gaps in clinical settings. When supplement visibility lives inside the same system as prescriptions, care coordination improves immediately. University Hospitals demonstrated this when EHR-linked supplement recommendations reduced fragmentation and improved safety coordination across care teams.
-
Connect to a digital dispensary for ordering and monitoring. Platforms that sit inside your clinical system allow patients to order directly and give your team real-time adherence data. First-fill rates and refill intervals are the most telling early indicators of whether a supplement protocol is actually being followed.
-
Run interaction checks before every recommendation. This step is non-negotiable. Many clinicians are surprised to learn that common polyphenols like quercetin and resveratrol can interact with warfarin and certain chemotherapy agents. Decision support tools automate this check, but your team needs to know how to interpret and act on the alerts generated.
-
Generate patient-friendly care plans using AI-assisted tools. Clinicians spend approximately 13 hours weekly on indirect care tasks, including supplement documentation and patient communication. AI tools that auto-generate plain-language summaries from clinical notes cut that time significantly while improving patient comprehension.
Pro Tip: When building protocol templates, include a field for “patient-reported supplement use at intake.” Patients frequently take supplements they do not mention unless directly asked. Capturing this data at the front end prevents undocumented interactions from emerging later.
Troubleshooting common workflow pitfalls
Even well-designed workflows break down in predictable places. Knowing where failure typically occurs puts your team ahead of the problem.

Documentation gaps are the most common and most consequential error. Missing a single required field, such as clinical indication or prescribing clinician name, can trigger a rejection during internal audit or delay an adverse event investigation at the worst possible moment. Embedding data completeness checks directly into your workflow, rather than relying on retrospective review, prevents these gaps from compounding.
Three additional failure points are worth specific attention:
- Skipping adherence tracking. Supplement protocols that lack a monitoring mechanism have no feedback loop. Without first-fill and refill data, you have no way to distinguish between a protocol that failed clinically and one that was never followed.
- Inconsistent adverse event reporting. Many clinical teams triage adverse events informally and only escalate the obvious cases. A formal triage protocol, moving from intake through seriousness determination to MedWatch submission, reduces missed or delayed safety reports and protects both the patient and the institution.
- Ignoring supplement-drug interactions in non-formulary products. If your decision support only covers formulary drugs, self-reported supplement use falls outside the check entirely. Close this gap by extending your interaction database to include common nutraceuticals.
“Well-designed adverse event intake, triage, and reporting processes transform regulatory obligations into manageable, structured clinical workflows.” — Adverse Event Reporting Workflow Perspectives
Training is frequently underestimated as a workflow component. Staff who do not understand why a documentation field matters are more likely to skip it under time pressure. Brief, protocol-specific training sessions, combined with EHR-based flags that alert staff to missing data in real time, produce far better compliance outcomes than annual general training modules.
For specialized populations, understanding nutrient-specific requirements can also shape how you design protocol templates. For example, bariatric patients have lifelong nutrient needs that require ongoing monitoring built directly into their care plan, not handled as a one-time recommendation.
You can also strengthen your team’s ability to assess supplements for clinical value by building evaluation criteria into the protocol selection process from the start.
Measuring workflow effectiveness over time
Designing the workflow is step one. Knowing whether it is working requires deliberate measurement.
Pro Tip: Review your supplement first-fill rates monthly. A rate below 70% is a strong signal that either the recommendation process lacks patient engagement or the ordering pathway creates too much friction.
The metrics below cover the full clinical supplement tracking spectrum, from patient behavior to regulatory compliance:
| Metric | Target Benchmark | What It Reveals |
|---|---|---|
| Supplement first-fill rate | 70% or above | Patient engagement and ordering friction |
| Adverse event reporting timeliness | 100% within 15 business days | Regulatory compliance posture |
| Documentation completeness rate | 95% or above at intake | Workflow discipline and audit readiness |
| Supplement-drug interaction check rate | 100% prior to recommendation | Safety protocol adherence |
| Patient adherence at 90 days | Tracked via dispensary data | Protocol effectiveness and follow-through |
Adherence data from digital dispensaries is the most underused asset in most clinical supplement workflows. Refill intervals tell you whether a patient is taking a supplement consistently, stopping early, or doubling up. That data should trigger proactive outreach, not just be reviewed at the next scheduled visit.
Regulatory compliance review deserves its own calendar slot. A quarterly review of all MedWatch submissions, along with a comparison of submission dates to intake dates, quickly reveals whether your 15-day reporting clock is being respected. Starting in October 2026, you will also need to verify that all electronic submissions comply with ICH E2B(R3) data requirements, including new mandatory data elements and formatting standards for ESG NextGen.
Automation reduces the variability that makes these audits stressful. Automated authorization workflows in radiation oncology settings reduced denial rates from 7.6% to 2.6% and shortened authorization times by 34%. The principle applies directly to supplement workflows: when policy-required data fields are built into the intake process and flagged automatically when missing, your audit results reflect system design rather than individual performance.
My perspective on where this work actually breaks down
I’ve seen a lot of clinical teams spend months selecting the right technology platform, only to discover that the real problem was upstream. Staff were skipping documentation fields because no one had explained their regulatory purpose. Interaction checks were configured but not reviewed because no one owned that responsibility in the workflow.
In my experience, the single most valuable thing you can do before deploying any new tool is to map who owns each step. Not the department. One person. When adverse event intake lacks a named owner, it defaults to whoever has time, which means it defaults to never.
What I’ve also learned is that the shift toward single-system supplement management inside EHRs is genuinely improving safety coordination, not just convenience. Clinicians who can see a patient’s supplement list in the same view as their medications catch interactions they would otherwise miss entirely.
The ICH E2B(R3) mandate is the compliance deadline that most supplement-adjacent clinical teams are not yet ready for. If your adverse event reporting process is still largely manual or uses an older electronic format, that is the highest-priority item on your workflow improvement list right now.
My practical advice: prioritize data completeness at intake, assign named owners to each workflow stage, and treat adherence monitoring as a clinical activity, not an administrative one. Patient safety in supplement management is built on process discipline, not product selection alone.
— cristopher
Supplements your clinical workflow can actually rely on
When you have invested in building a rigorous clinical supplement process, the quality of the products you recommend has to match the quality of your workflow. Superiorformulas was founded by a physician-scientist with exactly that gap in mind.
Every formulation in the Superiorformulas line is physician-developed, manufactured in GMP-certified facilities, and third-party tested for purity and potency. The product range covers longevity, cellular health, Nrf2 activation, and metabolic support, using clinically studied polyphenols, adaptogens, and phytonutrients with documented mechanisms. For clinicians who want to understand the science behind each formulation before recommending it, the research-backed supplement formulations page provides full transparency. When your workflow demands traceability, start with supplements built for it.
FAQ
What is a clinical supplement workflow?
A clinical supplement workflow is a structured process covering supplement recommendation, documentation, patient ordering, adherence monitoring, and adverse event reporting within a clinical setting. It follows the same governance principles applied to pharmaceutical workflows.
How does EHR integration improve supplement management?
Integrating supplement recommendations into EHR medication workspaces gives care teams full visibility into what patients are taking alongside prescribed drugs, reducing the risk of missed interactions and improving care coordination across providers.
What are the FDA reporting requirements for supplement adverse events?
Labeled manufacturers, packers, and distributors must submit MedWatch Form 3500A within 15 business days for serious adverse events. Starting October 1, 2026, electronic submissions must comply with ICH E2B(R3) data standards.
Which metrics should clinicians track to evaluate workflow performance?
Key metrics include supplement first-fill rate, adverse event reporting timeliness, documentation completeness at intake, and patient adherence at 90 days tracked through digital dispensary data.
How does automation reduce compliance risk in supplement workflows?
Embedding data completeness checks and policy requirements directly into workflow software flags missing information at intake rather than during review, reducing reporting delays and lowering the rate of incomplete or rejected adverse event submissions.



